Page 17 of 33
PH4.9 | PH4.9 | Heart Failure Pharmacotherapy — SDL Guide
Learning Objectives
- Explain the neurohormonal pathophysiology of heart failure and how it provides the rationale for each drug class used in HFrEF.
- Describe the pharmacokinetics, pharmacodynamics, therapeutic uses, and adverse drug reactions of drugs used for heart failure.
- Identify the four evidence-based drug classes that improve survival in HFrEF and the landmark trials supporting each.
- Devise a management plan for HFrEF and acute decompensated heart failure, and describe strategies to prevent long-term complications.
INSTRUCTIONS
Heart failure represents the final common pathway of almost every cardiac disease. The pharmacological management of HFrEF has been transformed in the past 30 years by a series of landmark trials — from CONSENSUS (enalapril) in 1987 to DAPA-HF (dapagliflozin) in 2019 — that have progressively added drug classes to the survival-improving toolkit. Today, four pillars are recognised: ACEi/ARNI, beta-blockers, mineralocorticoid receptor antagonists, and SGLT2 inhibitors. Understanding why these four classes survive when others fail requires understanding the neurohormonal cascade driving heart failure — which this SDL provides.
References
- Tripathi KD. Essentials of Medical Pharmacology, 9th ed., Ch. 38 (Cardiac Glycosides and Heart Failure) (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 14th ed., Ch. 28 (Pharmacotherapy of Congestive Heart Failure) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 62-year-old woman with a history of anterior MI 4 years ago is admitted with progressive breathlessness over 3 weeks — she now struggles to dress herself. Examination: HR 92, BP 100/70, raised JVP, bilateral basal crepitations, pitting oedema to mid-calves. Echocardiogram shows LVEF 28%, dilated LV with global hypokinesia. She is on furosemide 40 mg, atorvastatin 40 mg, aspirin 75 mg, and ramipril 2.5 mg. She is not on a beta-blocker — her referring doctor was concerned it would 'weaken the heart further.' Is the doctor correct? What should her optimised regimen include, and in what order do you introduce the drugs safely?
WHY THIS MATTERS
Heart failure affects over 64 million people worldwide and is the commonest cause of hospitalisation in adults over 65 in many countries. In India, it carries a particularly poor prognosis with 50% one-year mortality in advanced stages. Despite this, HFrEF is now the only major cardiac condition where adding drugs — specifically, four distinct drug classes — each independently reduces mortality. The doctor who withholds the beta-blocker out of concern about negative inotropy is making a common but dangerous error: in HFrEF, beta-blockers are not harmful — they are life-saving. Understanding why requires the neurohormonal framework this SDL builds.
RECALL
Recall from physiology and previous SDLs:
- Frank-Starling mechanism (PY): increased ventricular filling → increased stroke volume (within limits). In HF, this initially compensates for reduced EF but eventually, the overstretched ventricle operates on the descending limb of the Starling curve.
- Neurohormonal systems (PY): RAAS (renin → Ang II → aldosterone → Na retention + vasoconstriction + remodelling); sympathetic nervous system (↑catecholamines → ↑HR + ↑contractility + vasoconstriction); ADH/vasopressin (water retention). All three are activated in HF and all contribute to the disease's progression.
- ACEi/ARB mechanisms in cvs1-raas SDL; Diuretic mechanisms in cvs1-diuretics SDL; RAAS inhibitors across these SDLs.
- Cardiac glycosides (recall from BI): digitalis/digoxin inhibits Na-K-ATPase → increased intracellular Na → reduced Na-Ca exchange → increased intracellular Ca → positive inotropy. Also slows AV conduction (vagal).
Pathophysiology of Heart Failure: Neurohormonal Maladaptation
Heart failure is a clinical syndrome of impaired cardiac output relative to metabolic demands, characterised by symptoms of congestion and/or low output. The pharmacologically most relevant phenotype is HFrEF (heart failure with reduced ejection fraction) — defined as LVEF <40% — in which systolic dysfunction (weakened myocardium) is the primary abnormality. HFpEF (preserved EF, LVEF ≥50%) is the other major phenotype, characterised by diastolic dysfunction with a relatively intact LVEF; it affects a larger and predominantly elderly, obese, hypertensive, diabetic population.
In HFrEF, the impaired cardiac output triggers a cascade of compensatory neurohormonal responses that are initially adaptive but become progressively harmful — the pathological core of heart failure progression.
Step 1 — Compensatory activation: Reduced CO → reduced renal perfusion → RAAS activation (Ang II + aldosterone) → Na and water retention (↑preload via the Starling mechanism); simultaneously, sympathetic nervous system (SNS) activation → ↑HR and ↑contractility via catecholamines, and ↑peripheral vasoconstriction (↑afterload). ADH release adds to fluid retention.
Step 2 — Maladaptation: These initially helpful responses become chronically sustained, converting from compensation to harm: Ang II-mediated persistent vasoconstriction increases afterload beyond what the failing heart can overcome → further CO fall; aldosterone-driven Na retention → fluid overload → congestion; chronic catecholamine excess → down-regulation of β-receptors (desensitisation → ↓contractile response) + direct myocardial toxicity + pro-arrhythmic effects; Ang II and aldosterone directly drive ventricular remodelling — myocyte hypertrophy, apoptosis, and interstitial fibrosis → progressive ventricular dilatation and sphericisation → further EF reduction.
Step 3 — Pharmacological logic: Every drug class with proven mortality benefit in HFrEF interrupts a specific arm of this neurohormonal cascade: ACEi/ARNI block Ang II; beta-blockers block catecholamines; MRA blocks aldosterone; SGLT2i reduce preload + nephroprotection + cardiomyocyte protection. Drugs that merely address the symptom (diuretics, positive inotropes) without blocking neurohormonal activation generally do not prolong survival.
IMPORTANT: Cardiac remodelling is the structural enlargement and shape change of the LV under neurohormonal stress. The four survival drugs reverse remodelling — measurable as increased EF on serial echo — and this correlates with improved outcomes. Diuretics, despite being the most symptom-effective drugs, do not reverse remodelling.
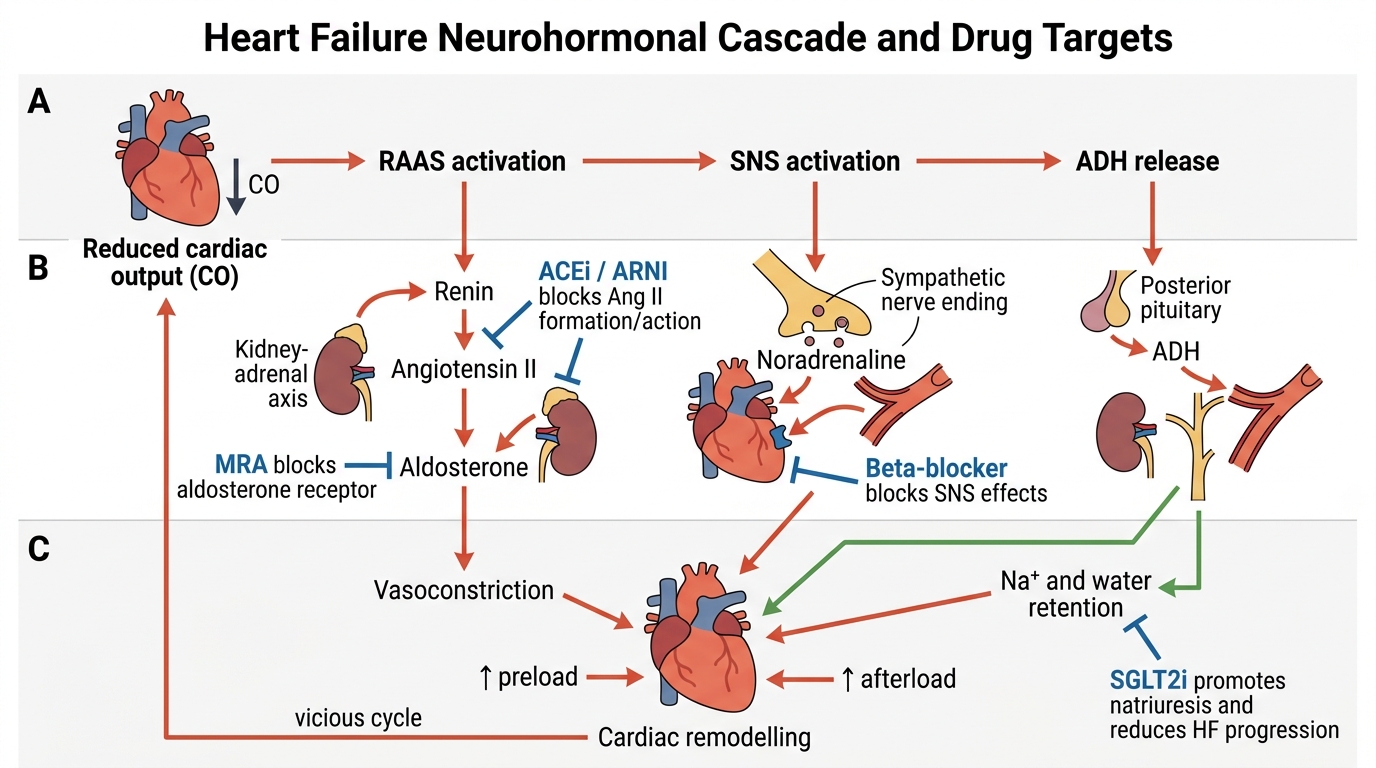
Heart Failure Neurohormonal Cascade and Drug Targets
Therapeutic Goals: Neurohormonal Blockade and Symptom Control
Heart failure pharmacotherapy pursues two distinct goals that must be managed simultaneously but addressed with different drug classes.
Goal 1 — Reduce mortality and prevent disease progression (neurohormonal blockade): The four-pillar drug classes — ACEi/ARNI, beta-blockers, MRA (aldosterone antagonists), and SGLT2 inhibitors — each independently reduce cardiovascular death, hospitalisation for HF, and sudden death. These benefits are additive: each class blocks a different neurohormonal axis. Starting all four at low doses is preferred over maximising one drug before adding the next. This is the most important pharmacological principle in HFrEF.
Goal 2 — Relieve symptoms and prevent congestion (fluid management and rate control): Loop diuretics reduce pulmonary and peripheral congestion (the primary cause of breathlessness and oedema in HF) but do NOT reduce mortality (may increase arrhythmias and RAAS counter-activation with aggressive use). Digoxin reduces symptoms and HF hospitalisation but not mortality in sinus rhythm HF (DIG trial). Ivabradine (I(f) inhibitor) reduces HF hospitalisation when HR remains >70 bpm despite maximally tolerated beta-blocker (SHIFT trial) — it does not worsen inotropy.
Strategies to prevent long-term complications of HFrEF:
- Sudden cardiac death (arrhythmia): The most common cause of death in mild–moderate HF. Beta-blockers, RAAS blockade, and MRA reduce sudden death via anti-remodelling and anti-arrhythmic effects. ICD (implantable cardioverter-defibrillator) is indicated for LVEF ≤35% on optimal medical therapy with life expectancy >1 year.
- Stroke (in AF): Atrial fibrillation is common in HF; anticoagulation with DOAC or warfarin is required in AF + HF (CHA₂DS₂-VASc ≥2).
- Progressive CKD: ACEi/ARB slow CKD progression; SGLT2i provide additional nephroprotection; loop diuretics must be carefully titrated to avoid diuretic-induced pre-renal AKI.
- Recurrent hospitalisation: Optimised medical therapy + patient education on daily weight monitoring + prompt treatment of decompensation reduces readmissions.
Classification of Heart Failure Drugs
Heart failure drugs are most clinically useful when classified by their evidence for mortality reduction versus purely symptom management.
MORTALITY-REDUCING DRUGS IN HFrEF (the four pillars):
1. ACEi (enalapril, ramipril, lisinopril) — or ARNI (sacubitril/valsartan) if switching from ACEi is feasible (PARADIGM-HF evidence).
2. Beta-blockers — specifically the THREE with proven HFrEF mortality benefit: carvedilol (COPERNICUS trial), bisoprolol (CIBIS-II trial), metoprolol succinate (MERIT-HF trial). NOT atenolol; NOT metoprolol tartrate (immediate-release — no survival data, may cause harm due to variable plasma levels).
3. Mineralocorticoid receptor antagonists (MRA) — spironolactone (RALES: HFrEF LVEF <35%) and eplerenone (EMPHASIS-HF: mild HFrEF NYHA II; EPHESUS: post-MI with HFrEF).
4. SGLT2 inhibitors — dapagliflozin (DAPA-HF, HFrEF, with and without T2DM) and empagliflozin (EMPEROR-Reduced for HFrEF; EMPEROR-Preserved for HFpEF — dual approval).
SYMPTOM-MANAGING DRUGS (HFrEF and HFpEF):
5. Loop diuretics — furosemide, torsemide (preferred for more predictable oral bioavailability in HF): relieve congestion (breathlessness, oedema); titrate to weight and symptoms; no mortality benefit.
6. Ivabradine — selective I(f) funny-current inhibitor in SA node; reduces HR without negative inotropy; SHIFT trial: reduced composite CV death + HHF in HFrEF with LVEF ≤35%, sinus rhythm, and HR ≥70 bpm on maximum tolerated beta-blocker.
7. Digoxin — positive inotrope (Na-K-ATPase inhibition) + vagally mediated AV node slowing; reduces HF hospitalisation and symptom severity but NOT mortality in sinus rhythm (DIG trial); narrow therapeutic index (0.5–0.9 ng/mL target).
ACUTE DECOMPENSATED HF (hospital only):
8. Dobutamine (β1 agonist): positive inotrope + mild vasodilator; used IV for acute low-output HF.
9. Dopamine (dose-dependent: <2 mcg/kg/min = dopaminergic → renal vasodilation; 2–5 = β1 → inotropy; >5 = α1 → vasoconstriction).
10. Milrinone (PDE3 inhibitor): positive inotrope + vasodilator; prolongs cAMP; IV; not for chronic use in HFrEF (increased mortality in PROMISE trial).
HFpEF pharmacotherapy: No drug has been proven to reduce mortality in HFpEF until empagliflozin (EMPEROR-Preserved, 2021). Standard management: diuretics for congestion, treat comorbidities (HTN, diabetes, AF), SGLT2i for empagliflozin-eligible patients. ACEi/ARBs/MRA have neutral effects in HFpEF trials.
SELF-CHECK
In a patient with HFrEF (LVEF 30%), which beta-blocker is recommended based on survival trial evidence?
A. Atenolol 50 mg once daily
B. Metoprolol tartrate (immediate-release) 25 mg twice daily
C. Bisoprolol 2.5 mg once daily (target 10 mg)
D. Propranolol 40 mg twice daily
Reveal Answer
Answer: C. Bisoprolol 2.5 mg once daily (target 10 mg)
Bisoprolol is one of the three beta-blockers with proven mortality benefit in HFrEF, demonstrated in the CIBIS-II trial. The other two are carvedilol (COPERNICUS) and metoprolol succinate (MERIT-HF). Atenolol has no HFrEF survival evidence; metoprolol tartrate (immediate-release) has no HFrEF survival trial support — only metoprolol succinate (extended-release) has this evidence (MERIT-HF). Propranolol (non-selective, lipophilic) has no HFrEF survival data and has the potential for adverse metabolic and CNS effects.