Page 18 of 33
PH4.9 | PH4.9 | Heart Failure Pharmacotherapy — SDL Guide (Part 2)
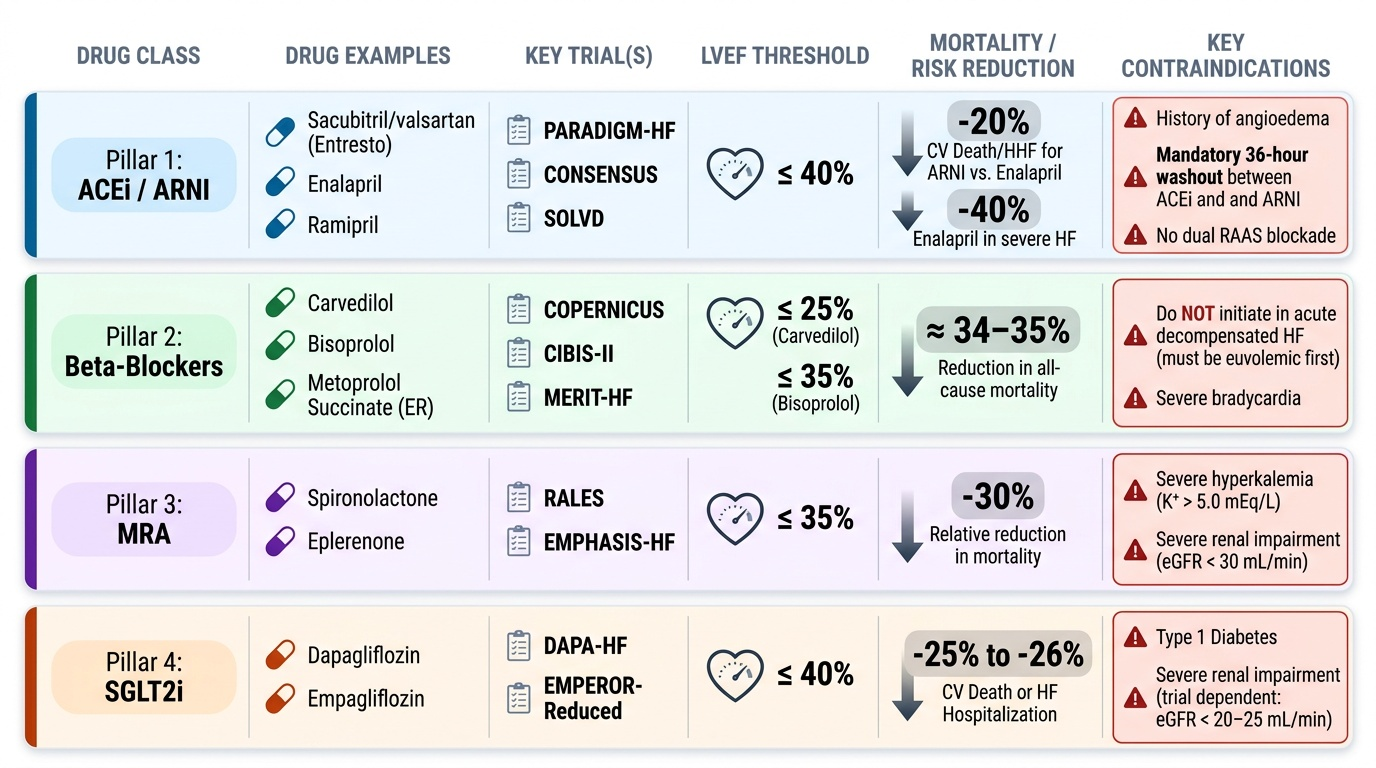
The Four Pillars: ACEi/ARNI, Beta-Blockers, MRA, and SGLT2i
The four-pillar approach to HFrEF represents the most robust evidence base in cardiovascular pharmacotherapy — each class independently reduces the composite of cardiovascular death and heart failure hospitalisation in large randomised controlled trials.
Pillar 1 — ACEi or ARNI: ACEi (enalapril, ramipril) were the first drugs to demonstrate survival benefit in HFrEF (CONSENSUS trial with enalapril, 1987: 40% mortality reduction in severe HF; SOLVD with enalapril in mild–moderate HF). The ARNI sacubitril/valsartan (Entresto) superseded ACEi in PARADIGM-HF (2014): compared to enalapril in HFrEF (LVEF ≤40%), sacubitril/valsartan reduced CV death + HHF by 20% — establishing ARNI as the preferred RAAS agent in HFrEF. Use ACEi or ARNI — NOT ARB as first-line in HFrEF (ARBs are second-line for RAAS inhibition when both ACEi and ARNI are not tolerated). The 36-hour washout from ACEi before ARNI initiation is mandatory to prevent dangerous dual bradykinin accumulation → angioedema.
Pillar 2 — Beta-Blockers: The most counterintuitive pillar — stimulating the sympathetically overdriven, catecholamine-exhausted heart with a beta-blocker seems paradoxical, yet the evidence is overwhelming. Chronic beta-blocker therapy in HFrEF: upregulates cardiac β1-receptors (restoring responsiveness), reverses adverse remodelling (increases LVEF over months), reduces sudden cardiac death, and improves exercise tolerance. The three proven agents:
- Carvedilol (COPERNICUS): non-selective β1+β2+α1 blocker; reduces mortality in severe HFrEF (LVEF ≤25%).
- Bisoprolol (CIBIS-II): selective β1; reduces mortality in moderate–severe HFrEF.
- Metoprolol succinate (MERIT-HF): selective β1, extended-release; reduces mortality; the only metoprolol formulation with HFrEF evidence.
Important: Never initiate beta-blockers in acute decompensated HF — wait until the patient is euvolaemic and haemodynamically stable (no signs of congestion, adequate BP, no inotrope need). This is why the opening case's doctor was partially correct — the timing mattered. Start at very low doses (carvedilol 3.125 mg BD; bisoprolol 1.25 mg OD; metoprolol succinate 12.5 mg OD) and up-titrate slowly over weeks.
Pillar 3 — Mineralocorticoid Receptor Antagonists (MRA): Spironolactone and eplerenone block aldosterone's adverse cardiac effects (fibrosis, inflammation, remodelling) beyond their diuretic action. Key trials:
- RALES (spironolactone 25 mg in HFrEF LVEF <35% + ACEi + loop diuretic): 30% reduction in all-cause mortality.
- EMPHASIS-HF (eplerenone in mild HFrEF NYHA class II, LVEF <35%): 37% reduction in composite CV death + HHF.
- EPHESUS (eplerenone post-MI with HFrEF or diabetes): 15% mortality reduction.
Risk: hyperkalaemia — monitor K and creatinine at 1 week, 1 month, 3 months after initiation. Avoid when K >5.0 mEq/L or eGFR <30 mL/min/1.73m². Spironolactone at high doses causes gynaecomastia (anti-androgenic); eplerenone is more MR-selective and avoids this.
Pillar 4 — SGLT2 inhibitors: Sodium-glucose cotransporter-2 inhibitors were developed for diabetes but demonstrated remarkable HF benefits independent of glycaemic effects:
- DAPA-HF (dapagliflozin 10 mg in HFrEF LVEF <40%, with AND without T2DM): 26% reduction in composite worsening HF or CV death vs placebo.
- EMPEROR-Reduced (empagliflozin in HFrEF): similar magnitude reduction.
- EMPEROR-Preserved (empagliflozin in HFpEF, LVEF >40%): first drug to show significant benefit in HFpEF (reduced HF hospitalisation) — a landmark, because most previous HFpEF trials were neutral.
Mechanism in HF (beyond glycaemia): osmotic diuresis + natriuresis → ↓preload; cardioprotective effects (↓inflammation, ↓fibrosis, ↑mitochondrial function); nephroprotective effects. SGLT2i are approved for HF regardless of diabetes status and can be initiated at eGFR ≥20–25 (lower threshold for HF indication vs glycaemic indication ~45).
Provided image
Symptom Management and Hospitalised HF: Diuretics, Digoxin, and Inotropes
While the four pillars provide the survival framework, the symptom-managing drugs are indispensable for quality of life and acute decompensation management.
Loop diuretics — furosemide, torsemide: The primary agents for relieving congestion in HF. Torsemide is preferred over furosemide by many HF experts because of its better and more predictable oral bioavailability (80–90% vs 50–70% for furosemide) — particularly important in HF, where gut wall oedema impairs oral furosemide absorption (the reason IV furosemide works better acutely). Loop diuretics reduce pulmonary capillary wedge pressure, relieve dyspnoea, and reduce oedema — but do NOT reverse neurohormonal activation and may activate RAAS (reducing their own efficacy over time). Patients on chronic loop diuretics who gain >2 kg in 2 days (from retained fluid) should double their diuretic dose temporarily (self-management titration).
Ivabradine (I(f) channel inhibitor): The funny current (I(f)) in the SA node pacemaker cells determines the spontaneous diastolic depolarisation rate — it is the intrinsic pacemaker current. Ivabradine selectively blocks this channel → slower diastolic depolarisation → reduced HR — without affecting contractility (no inotropy), conduction, or blood pressure. This is mechanistically distinct from beta-blockers. SHIFT trial: ivabradine + background beta-blocker therapy in HFrEF with LVEF ≤35% and HR ≥70 bpm in sinus rhythm → 18% reduction in composite CV death + HHF. Indication: HFrEF, NYHA II–IV, sinus rhythm, HR ≥70 bpm, despite maximally tolerated beta-blocker. Adverse effects: visual phosphenes (transient luminous phenomena), mild bradycardia.
Digoxin (cardiac glycoside): Mechanism: inhibits Na-K-ATPase (the sodium pump) in cardiomyocytes → intracellular Na accumulates → Na-Ca exchanger pumps less Ca out → intracellular Ca increases → positive inotropy (more Ca available for troponin-C binding during systole). Also increases vagal tone → slows AV conduction (useful for rate control in AF with HF). The DIG trial showed digoxin reduces HF hospitalisation and improves symptoms but does NOT reduce mortality in HF with sinus rhythm — this is a critical distinction from the four-pillar drugs. In AF + HFrEF, digoxin is used as rate control adjunct.
Narrow therapeutic index: digoxin target plasma level is 0.5–0.9 ng/mL for HF — levels above 1.5 ng/mL are associated with toxicity. At levels >1.0 ng/mL, mortality risk increases (post-hoc analysis of DIG trial). Digoxin toxicity signs: cardiac — bradycardia, AV block, ventricular arrhythmias (paroxysmal atrial tachycardia with block is pathognomonic); non-cardiac — visual disturbances (yellow-green vision, halos), GI (anorexia, nausea, vomiting), CNS (confusion). Precipitating factors: hypokalaemia (loop diuretics → ↓K → digoxin binds more avidly to K-depleted Na-K-ATPase → toxicity at therapeutic levels), hypomagnesaemia, renal impairment (digoxin renally excreted — reduce dose in CKD). Drug interactions: amiodarone, verapamil, quinidine all increase digoxin levels (block tubular secretion and/or reduce distribution).
Acute inotropic support (hospital only): In patients with acute decompensated HF or cardiogenic shock with low CO despite optimal therapy:
- Dobutamine (selective β1 agonist): increases contractility and heart rate; mild vasodilation (β2); improves CO; no α1 vasoconstriction at standard doses. Used IV for stabilisation — not for chronic use.
- Dopamine (dose-dependent effects): at <2 mcg/kg/min — dopaminergic receptors → renal and mesenteric vasodilation (↑renal perfusion); 2–5 mcg/kg/min — β1 → positive inotropy; >5–10 mcg/kg/min — α1 → vasoconstriction (increases afterload — potentially harmful in HF).
- Milrinone (PDE3 inhibitor): IV inodilator (positive inotrope + vasodilator); may be preferred over dobutamine when patient is on beta-blocker (milrinone's mechanism is downstream of the β receptor). PROMISE trial showed chronic oral PDE3 inhibitors increase mortality — IV short-term use only.
SELF-CHECK
A patient with HFrEF (LVEF 28%) in sinus rhythm with HR 88 bpm remains symptomatic (NYHA III) despite optimal doses of sacubitril/valsartan, carvedilol 25 mg BD, and spironolactone 25 mg OD. Dapagliflozin has just been added. The next most appropriate drug to consider adding is:
A. Digoxin 0.125 mg once daily
B. Ivabradine 5 mg twice daily
C. Furosemide 80 mg once daily (doubling the current dose)
D. Metoprolol succinate in addition to carvedilol
Reveal Answer
Answer: B. Ivabradine 5 mg twice daily
This patient is on all four pillars (ARNI, beta-blocker, MRA, SGLT2i) but remains symptomatic with HR 88 bpm in sinus rhythm. Ivabradine is indicated in HFrEF with LVEF ≤35%, sinus rhythm, HR ≥70 bpm, despite maximally tolerated beta-blocker — it reduces HHF (SHIFT trial) without affecting inotropy. Digoxin reduces HF hospitalisation but has a narrow therapeutic index and no survival benefit — it would be a less preferred addition when ivabradine is available. Doubling furosemide addresses congestion but does not address the ongoing high HR risk. Two beta-blockers should never be combined (additive bradycardia/AV block without additive benefit).
CLINICAL PEARL
The 'beta-blocker initiation' conversation — dispelling the myth: The fear that beta-blockers will worsen HFrEF is one of the most persistent and harmful misconceptions in internal medicine. The resolution is simple: (1) TIMING — never initiate a beta-blocker during acute decompensation or if the patient is receiving IV inotropes; wait until euvolaemic and haemodynamically stable. (2) DOSE — start at the lowest dose and double every 2 weeks as tolerated; a small HR increase at first is expected. (3) FORMULATION — only carvedilol, bisoprolol, and metoprolol SUCCINATE have evidence; do not substitute atenolol or metoprolol tartrate. (4) MECHANISM — the short-term negative inotropic effect is outweighed by the long-term β-receptor upregulation, reverse remodelling, and anti-arrhythmic protection. The opening patient's beta-blocker was withheld incorrectly — once her acute decompensation is resolved and she is euvolaemic, carvedilol 3.125 mg BD should be started and titrated slowly.
Clinical Decision-Making: HF Management Plan and Long-Term Complication Prevention
An effective HFrEF management plan combines evidence-based mortality reduction with symptom control, monitoring, and long-term complication prevention.
Stepwise initiation of four-pillar therapy (stable outpatient HFrEF):
1. Start ACEi at low dose (enalapril 2.5 mg BD) or ARNI if affordable; uptitrate to target dose over 4–6 weeks.
2. Add loop diuretic for congestion (furosemide 20–40 mg) — titrate to symptoms and daily weight.
3. Once euvolaemic and stable: start beta-blocker at low dose (carvedilol 3.125 mg BD); uptitrate every 2 weeks.
4. Add MRA (spironolactone 25 mg or eplerenone 25 mg) once stable on ACEi + BB; monitor K and creatinine at 1 week, 1 month.
5. Add SGLT2i (dapagliflozin 10 mg or empagliflozin 10 mg); check eGFR and glucose at start.
6. If HR still ≥70 bpm on maximum tolerated beta-blocker in sinus rhythm: consider ivabradine.
7. Consider switching ACEi to ARNI when clinically stable.
Acute decompensated HF (in-hospital management):
- IV loop diuretic (furosemide IV 40–80 mg stat; then infusion or BD bolus to achieve urine output ≥100 mL/h)
- IV vasodilator (nitroglycerin IV, isosorbide IV) if systolic BP >90 mmHg — reduces preload
- If severe low CO/cardiogenic shock: IV dobutamine or IV milrinone; intra-aortic balloon pump
- Do NOT start beta-blocker acutely; do NOT stop chronic beta-blocker abruptly (rebound risk)
- Monitor: daily weight, electrolytes daily (K, creatinine), BP, urine output
Strategies to prevent long-term complications:
- Sudden death: beta-blockers, MRA (anti-fibrotic), amiodarone (for sustained ventricular arrhythmias); ICD for LVEF ≤35% on optimal medical therapy ≥3 months with NYHA II–III.
- Stroke in AF: DOACs preferred (apixaban, rivaroxaban) or warfarin for AF + HFrEF.
- CKD progression: ACEi/ARB/ARNI + SGLT2i provide nephroprotection; avoid NSAIDs; monitor creatinine + electrolytes.
- Worsening HF: patient-driven daily weight monitoring (action weight 2 kg above dry weight = increase diuretic dose); nurse-led telephone review; HF clinic follow-up.
- Device therapy: CRT (cardiac resynchronisation therapy — biventricular pacing) for LVEF ≤35%, NYHA II–III, QRS ≥150 ms with LBBB pattern — reduces HHF and mortality and improves EF.
SELF-CHECK
A patient on digoxin 0.125 mg daily for HFrEF develops anorexia, nausea, and bradycardia. His serum K is 2.9 mEq/L (furosemide 40 mg prescribed). Serum digoxin level is 1.8 ng/mL. What is the most likely explanation for digoxin toxicity?
A. The digoxin dose is too low — needs to be increased
B. Furosemide-induced hypokalaemia reduced binding competition at Na-K-ATPase, increasing digoxin's toxic effect
C. The patient has taken an overdose of digoxin
D. Digoxin toxicity is always caused by renal failure
Reveal Answer
Answer: B. Furosemide-induced hypokalaemia reduced binding competition at Na-K-ATPase, increasing digoxin's toxic effect
Hypokalaemia (K 2.9 mEq/L from furosemide) is the most important precipitant of digoxin toxicity at 'therapeutic' digoxin levels. Potassium normally competes with digoxin for binding to the K-site on Na-K-ATPase. When potassium is low, there is less competition → digoxin binds more avidly to a greater proportion of Na-K-ATPase pumps → toxic effects at levels that would be non-toxic in a normokalaemic patient. The target digoxin level for HF is 0.5–0.9 ng/mL; levels above 1.5 ng/mL risk toxicity even without hypokalaemia. Management: stop digoxin, correct hypokalaemia (IV/oral KCl), cardiac monitoring. If arrhythmia is severe: digoxin-specific antibody fragments (Digibind).
Self-Assessment: Heart Failure Drug Selection and Monitoring
Consolidate your understanding with the following reference tables.
Four-pillar trial summary:
| Pillar | Drug(s) | Key Trial | Population | Benefit |
|---|---|---|---|---|
| ACEi | Enalapril | CONSENSUS, SOLVD | HFrEF | 40% mortality ↓ (CONSENSUS) |
| ARNI | Sacubitril/valsartan | PARADIGM-HF | HFrEF LVEF ≤40% | 20% ↓CV death+HHF vs enalapril |
| Beta-blocker | Carvedilol | COPERNICUS | HFrEF LVEF <25% | 35% mortality ↓ |
| Beta-blocker | Bisoprolol | CIBIS-II | HFrEF | 34% mortality ↓ |
| Beta-blocker | Metoprolol succinate | MERIT-HF | HFrEF | 34% mortality ↓ |
| MRA | Spironolactone | RALES | HFrEF LVEF <35% | 30% mortality ↓ |
| MRA | Eplerenone | EMPHASIS-HF | HFrEF NYHA II | 37% ↓CV death+HHF |
| SGLT2i | Dapagliflozin | DAPA-HF | HFrEF ± T2DM | 26% ↓worsening HF+CV death |
| SGLT2i | Empagliflozin | EMPEROR-Preserved | HFpEF LVEF >40% | ↓HHF (first HFpEF drug) |
Digoxin toxicity monitoring:
- Target level: 0.5–0.9 ng/mL (measure 6–8 h post-dose)
- Precipitants: hypokalaemia, hypomagnesaemia, CKD, hypothyroidism, elderly (reduced volume of distribution), drug interactions (amiodarone, verapamil, quinidine — all increase digoxin level)
- Toxicity signs: bradycardia, AV block, PAT with block, VT, yellow-green vision, GI symptoms
- Treatment: stop digoxin, correct K/Mg, cardiac monitoring; Digibind (anti-digoxin Fab fragments) for life-threatening arrhythmias