Page 1 of 13
PH5.1 | PH5.1 | Obstructive Airway Disease Pharmacotherapy — SDL Guide
Learning Objectives
- Devise a stepwise pharmacological management plan for bronchial asthma across GINA stages
- Explain the rationale for COPD pharmacotherapy using the GOLD ABCD framework
- Describe the salient pharmacokinetics and pharmacodynamics of beta-2 agonists, anticholinergics, inhaled corticosteroids, leukotriene modifiers, methylxanthines, and biologics
- Enumerate clinically important adverse drug reactions and contraindications for each drug class
- Outline the pharmacotherapy of allergic rhinitis, including the most effective drug class and the rhinitis medicamentosa risk with topical decongestants
INSTRUCTIONS
Obstructive airway diseases — asthma, COPD, and rhinitis — together affect hundreds of millions of people globally and are among the most common reasons for hospital admission, emergency visits, and long-term disability. As a Year-2 pharmacology student, mastering this module means being able to match the right drug class to the right disease stage and patient, understand the safety boundaries (especially the asthma–LABA boxed warning and theophylline's narrow therapeutic window), and explain the mechanism behind every choice. This SDL builds systematically from pathophysiology through to stepwise clinical algorithms.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed. Jaypee Brothers, 2019. Chapters 16–17 (Respiratory & Antihistamine) (textbook)
- Brunton LL et al. Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed. McGraw-Hill, 2018. Chapter 34 (Pulmonary Pharmacology) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 24-year-old college student is brought to the emergency department at midnight, unable to complete a sentence. She has been using her salbutamol inhaler every 30 minutes for the past three hours with minimal relief. On examination: RR 28/min, SpO2 88% on room air, widespread expiratory wheeze, accessory muscle use. Her mother mentions she stopped her 'brown inhaler' three weeks ago because 'the attack was over.' Her peak flow is 35% of predicted. What is the immediate drug management, and what critical error in long-term therapy led to this near-fatal exacerbation?
WHY THIS MATTERS
Obstructive airway diseases are among the most prevalent chronic conditions you will encounter in general practice, internal medicine, paediatrics, and emergency care. Asthma affects approximately 300 million people worldwide; COPD is the third leading cause of death globally; allergic rhinitis affects 40% of the population and is often the upstream trigger that worsens co-existing asthma. The clinical stakes are high: under-treating asthma leads to preventable deaths, while over-treating COPD with ICS raises pneumonia risk. A systematic understanding of the drug classes, their mechanistic rationale, and their indication-specific boundaries is not academic preparation — it is the practical toolkit for every patient encounter involving respiratory complaints.
RECALL
Before proceeding, activate these building blocks from your Year-1 studies:
- Beta-2 adrenoceptors in bronchial smooth muscle: Gs-coupled, activate adenylyl cyclase → ↑cAMP → PKA activation → smooth muscle relaxation. Recall why beta-2 selectivity matters (beta-1 stimulation = cardiac effects).
- Muscarinic (M3) receptors in airway: Gq-coupled, increase IP3 and DAG → smooth muscle contraction + mucus secretion. Blockade with anticholinergics relieves this.
- Arachidonic acid pathway: phospholipase A2 → arachidonic acid → 5-lipoxygenase (5-LOX) pathway → leukotrienes (LTC4, LTD4, LTE4 = cysteinyl leukotrienes, potent bronchoconstrictors). This is the target of leukotriene modifiers.
- IgE-mediated (Type I) hypersensitivity: antigen → IgE binding to mast cell Fcε receptors → degranulation → histamine, leukotrienes, prostaglandins → early and late phase bronchospasm. The target of anti-IgE biologics.
- Corticosteroid mechanism: bind cytoplasmic glucocorticoid receptor → translocate to nucleus → upregulate anti-inflammatory genes, downregulate cytokine/chemokine genes. Reduces eosinophilic inflammation in asthma.
Pathophysiology of Obstructive Airway Disease
Understanding the pathophysiology of obstructive airway diseases is the essential foundation for rational drug selection, because every drug class was designed to interrupt a specific pathological step. In bronchial asthma, the dominant process is chronic eosinophilic airway inflammation superimposed on bronchial hyper-reactivity. Allergen exposure triggers IgE-mediated mast cell degranulation, releasing histamine, cysteinyl leukotrienes (LTC4, LTD4, LTE4), and prostaglandins. These mediators cause immediate bronchoconstriction (the 'early-phase response'), followed 6–12 hours later by a cytokine-driven 'late-phase response' dominated by eosinophil recruitment. Interleukin-4 (IL-4) and IL-13 drive IgE class switching; IL-5 drives eosinophil production and survival; IL-4Rα signals are shared by both IL-4 and IL-13. Repeated inflammatory cycles lead to airway remodelling: subepithelial fibrosis, goblet cell metaplasia, smooth muscle hypertrophy, and angiogenesis — producing fixed obstruction on top of variable obstruction.
Chronic obstructive pulmonary disease (COPD) has a fundamentally different pathobiology. It is driven primarily by cigarette smoke–induced neutrophilic and macrophage-mediated inflammation rather than eosinophilic inflammation. The resulting protease-antiprotease imbalance destroys alveolar walls (emphysema) and/or causes goblet cell hyperplasia and excess mucus production (chronic bronchitis). Unlike asthma's largely reversible obstruction, COPD obstruction is largely irreversible and progressively worsens. The ratio of FEV1 to FVC falls below 0.70 post-bronchodilator (the GOLD criterion). The dominant symptom complex — dyspnoea, chronic productive cough, and recurrent exacerbations — reflects both airflow limitation and mucus plugging.
Allergic rhinitis shares the IgE-mediated mast cell mechanism of asthma but is localised to the nasal mucosa. Histamine is quantitatively more important in rhinitis (causing sneezing, pruritus, and rhinorrhoea) than in asthma, which is why H1 antihistamines are more effective in rhinitis than in asthma. Persistent nasal inflammation from rhinitis causes post-nasal drip, impairs mucociliary clearance, and frequently triggers asthma exacerbations — the 'united airway disease' concept. Recognising this upstream–downstream relationship is essential for prescribing: treating rhinitis often reduces the frequency of asthma attacks.
Image placeholder for the comparative diagram:
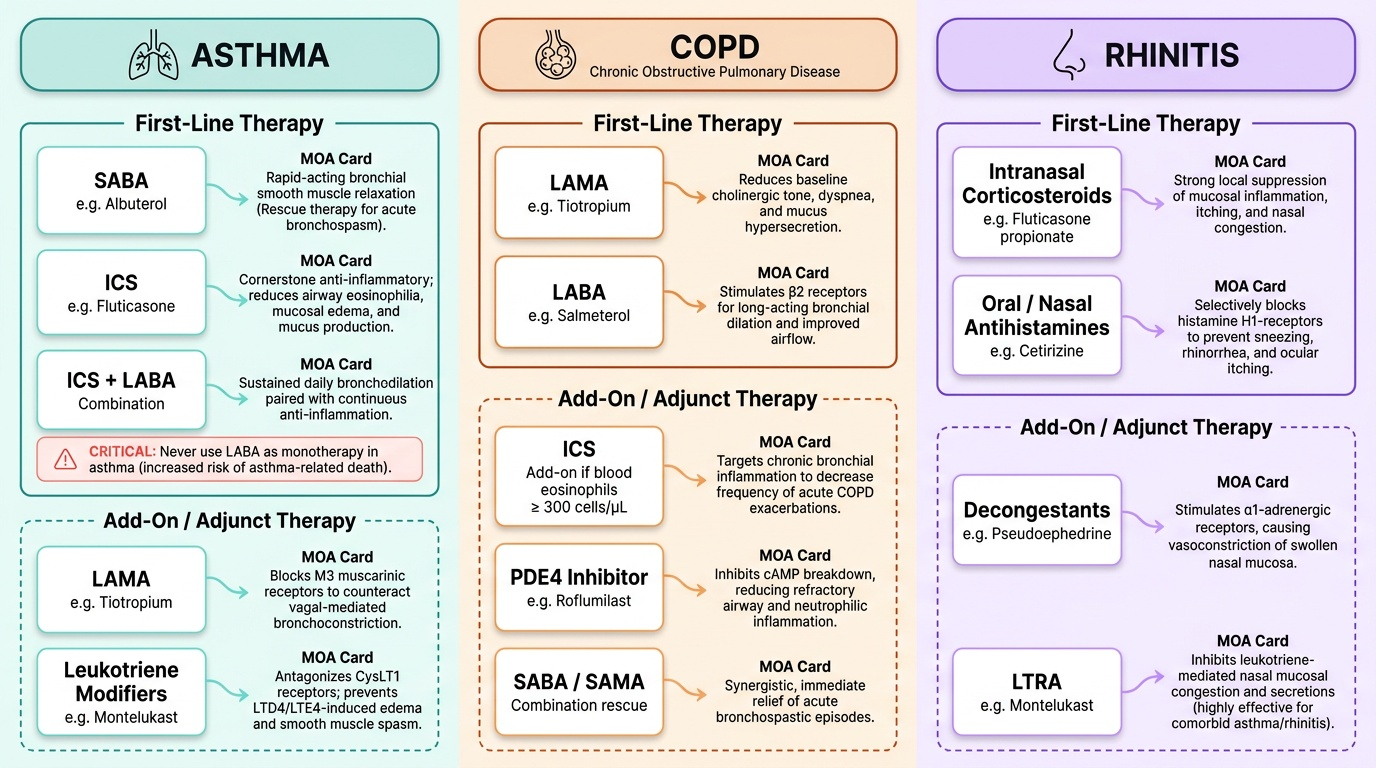
Provided image
SELF-CHECK
In bronchial asthma, which interleukin is primarily responsible for driving eosinophil production and survival, making it the target of mepolizumab and reslizumab?
A. IL-4
B. IL-5
C. IL-13
D. IL-6
Reveal Answer
Answer: B. IL-5
IL-5 is the principal cytokine driving eosinophil production from bone marrow, eosinophil activation, and survival in the airway. Mepolizumab and reslizumab are anti-IL-5 monoclonal antibodies; benralizumab targets the IL-5 receptor α-chain (IL-5Rα). IL-4 and IL-13 drive IgE class switching and mucus production — targets of dupilumab (anti-IL-4Rα). IL-6 is not a primary target in asthma biologic therapy.
Therapeutic Goals in Asthma, COPD, and Rhinitis
Before selecting a drug, a clinician must define what they are trying to achieve — because the therapeutic goals differ substantially across the three obstructive airway conditions, and the choice of drug class is directly determined by these goals. Conflating the goals leads to prescribing errors: the commonest one is applying ICS-LABA combination principles from asthma management uncritically to COPD, where the safety and efficacy calculus is different.
In bronchial asthma, the GINA (Global Initiative for Asthma) framework defines two paired goals. The first is control of current symptoms: minimising daytime and nocturnal symptoms, enabling normal activity and exercise, and achieving normal (or best attainable) peak expiratory flow. The second is reduction of future risk: preventing exacerbations, avoiding fixed airflow limitation from remodelling, and minimising treatment side effects. These two goals explain why short-acting bronchodilators alone are insufficient maintenance therapy — they address symptoms but do nothing to attenuate inflammation and remodelling. Hence inhaled corticosteroids, the cornerstone of asthma control therapy, are mandatory from Step 2 onward.
In COPD, the GOLD (Global Initiative for Chronic Obstructive Lung Disease) framework sets goals of relieving symptoms, improving exercise tolerance and health status, preventing and treating exacerbations, and reducing mortality in select subgroups. Critically, COPD is an irreversible disease — the goal of 'preventing remodelling' does not apply; instead, slowing the rate of FEV1 decline and reducing exacerbation frequency are the measurable targets. Bronchodilators (LABA, LAMA, or both) are the cornerstone of COPD maintenance because they directly address the fixed airflow limitation. ICS is added selectively for patients with high exacerbation frequency or eosinophilic features (blood eosinophils ≥300 cells/µL) — not universally, because of the pneumonia risk.
In allergic rhinitis, the goals are symptom relief (sneezing, rhinorrhoea, nasal congestion, pruritus) and prevention of complications (sinusitis, otitis media, sleep disruption, and triggering of lower-airway disease). The most effective single-agent class is intranasal corticosteroids — they address all four symptom domains, unlike antihistamines (which miss congestion) or decongestants (which address only congestion). Allergen avoidance, when practicable, is the only disease-modifying non-pharmacological intervention.
Drug Classification for Obstructive Airway Disease
A clear taxonomy of drug classes is the structural foundation for all subsequent learning in this module. Rather than memorising individual drugs in isolation, understanding the class architecture allows you to predict mechanism, use, and ADR profile for any agent within a class, and to reason about which class addresses which pathological step in the disease cascade. Each drug class exists because a specific pathological mechanism was identified as a therapeutic target — bronchospasm, inflammation, leukotriene excess, IgE-mediated mast cell activation — and a drug was designed or repurposed to interrupt that mechanism at the appropriate point. When the taxonomy is internalised, clinical prescribing decisions become logical deductions rather than memorised lists. The following overview maps each condition to its pharmacological toolkit, providing the conceptual structure that underpins the detailed per-class pharmacology in subsequent sections.
For asthma, the drug classes span five mechanistic categories:
1. Beta-2 agonists — bronchodilators acting on airway smooth muscle; subdivided into short-acting (SABA, for rescue) and long-acting (LABA, always with ICS in asthma — never as monotherapy due to a boxed warning for increased asthma-related deaths).
2. Inhaled corticosteroids (ICS) — the cornerstone anti-inflammatory agents; reduce airway eosinophilia, mucus production, and prevent remodelling.
3. Muscarinic antagonists (SAMA/LAMA) — anticholinergics that block M3-receptor–mediated bronchoconstriction and mucus secretion; ipratropium (SAMA) as add-on in acute severe asthma, tiotropium (LAMA) as add-on in difficult-to-treat asthma.
4. Leukotriene modifiers — CysLT1 receptor antagonists (montelukast, zafirlukast) block LTD4/LTE4-mediated bronchoconstriction; zileuton inhibits 5-LOX to prevent leukotriene synthesis upstream.
5. Methylxanthines (theophylline) and biologics (omalizumab, mepolizumab/reslizumab/benralizumab, dupilumab) — reserve/severe-asthma agents.
For COPD, the primary classes are:
1. Long-acting bronchodilators — LABA (salmeterol, formoterol, indacaterol, vilanterol) and LAMA (tiotropium, glycopyrronium, umeclidinium); these are the cornerstone, used alone or in combination (LABA-LAMA).
2. ICS-LABA combinations — added selectively for frequent exacerbators or eosinophilic COPD; carries a pneumonia risk not seen in asthma.
3. PDE4 inhibitors — roflumilast, for severe COPD with chronic-bronchitis phenotype and frequent exacerbations; reduces airway inflammation and exacerbation frequency.
4. Short-acting bronchodilators (SABA, SAMA) — for rescue and acute exacerbations.
For rhinitis:
1. Intranasal corticosteroids — most effective class; reduce all four symptom domains.
2. 2nd-generation H1 antihistamines — cetirizine, loratadine, fexofenadine (non-sedating); effective for sneezing, pruritus, rhinorrhoea; less effective for congestion.
3. Decongestants — topical (oxymetazoline, xylometazoline, ≤5 days) and oral (pseudoephedrine); topical overuse causes rebound congestion (rhinitis medicamentosa).
4. Cromolyn sodium — mast cell stabiliser; mild-moderate rhinitis, safe in pregnancy.
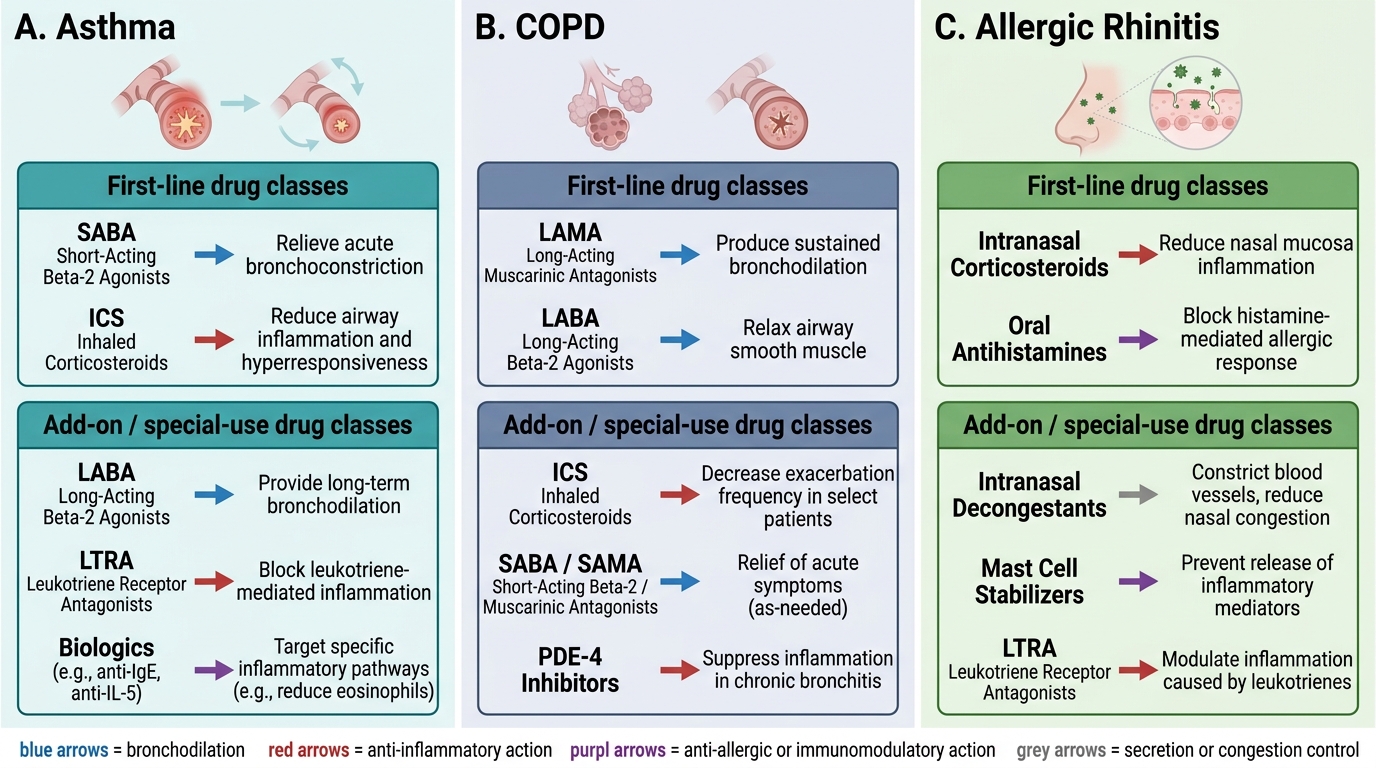
Drug Classes and Mechanisms in Asthma, COPD, and Rhinitis