Page 2 of 13
PH5.1 | PH5.1 | Obstructive Airway Disease Pharmacotherapy — SDL Guide (Part 2)
Bronchodilators: Beta-2 Agonists (SABA and LABA)
Beta-2 agonists are the most widely used bronchodilators in obstructive airway disease. They act on beta-2 adrenoceptors located in bronchial smooth muscle (Gs-coupled, ↑cAMP → PKA → smooth muscle relaxation), mast cells (suppresses mediator release), and mucociliary epithelium (increases ciliary beat frequency). The critical clinical differentiation is between short-acting (SABA) and long-acting (LABA) agents — a distinction that carries profound implications for safety in asthma.
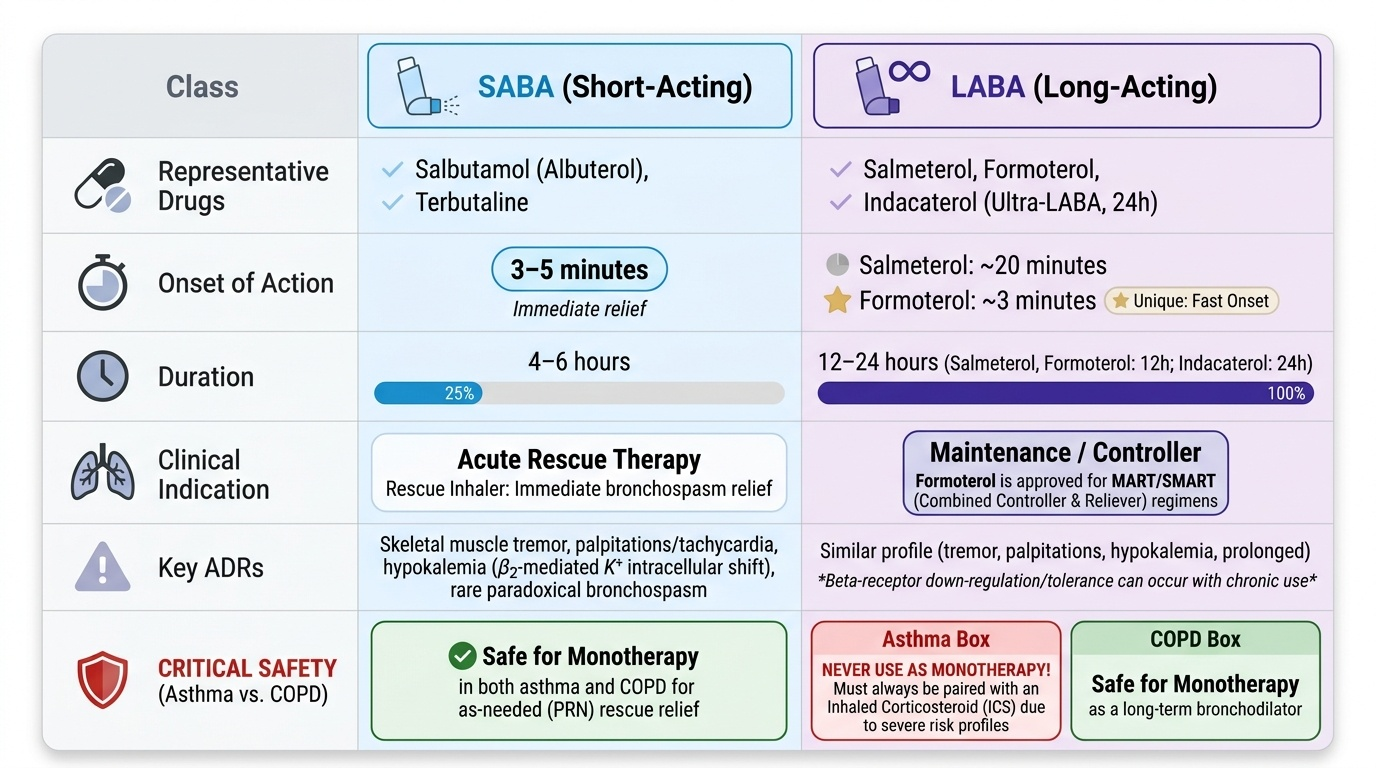
Short-acting beta-2 agonists (SABA): The prototypes are salbutamol (albuterol) and terbutaline. Their onset is 3–5 minutes, peak effect at 30–90 minutes, and duration 4–6 hours. They are inhaled via MDI or nebuliser for acute bronchospasm relief — the 'rescue inhaler' in asthma. In COPD, SABA is used on demand for symptom relief. Key pharmacokinetic point: inhaled delivery achieves high local concentration in the airway with low systemic absorption, limiting systemic beta-2 ADRs. ADRs include fine tremor (skeletal muscle beta-2 stimulation), palpitations and tachycardia (mild beta-1 spillover), hypokalaemia (beta-2 stimulation shifts K+ intracellularly), and paradoxical bronchospasm (rare, from propellant sensitivity).
Long-acting beta-2 agonists (LABA): The primary agents are salmeterol and formoterol. Salmeterol has delayed onset (~20 min) and 12-hour duration. Formoterol is unique: it has a fast onset comparable to SABA (~3 min) and a 12-hour duration — making it usable as both a reliever and controller (the basis of SMART/MART therapy). Indacaterol is an ultra-LABA (once-daily, 24-hour duration), approved for COPD. Critical safety rule for asthma: LABA must NEVER be used as monotherapy in asthma. The SMART trial demonstrated increased asthma-related deaths with salmeterol monotherapy. Current boxed warning: LABA must always be combined with ICS in asthma. In COPD, LABA monotherapy is entirely appropriate for long-term bronchodilation without this restriction.
ADRs of LABA: same class as SABA but potentially more prolonged — tremor, palpitations, hypokalaemia. Tolerance to some effects (bronchodilation is maintained longer than cardiovascular effects).
Provided image
SELF-CHECK
A 45-year-old man with COPD is prescribed formoterol monotherapy as a long-acting bronchodilator. A junior doctor objects, citing the LABA monotherapy warning. Who is correct?
A. The junior doctor — LABA monotherapy is contraindicated in all obstructive airway disease
B. The prescriber — the LABA monotherapy boxed warning applies specifically to asthma, not COPD
C. Neither — formoterol is only approved for asthma as a short-acting reliever
D. Both — LABA-LAMA combination is always needed; monotherapy of either is inadequate
Reveal Answer
Answer: B. The prescriber — the LABA monotherapy boxed warning applies specifically to asthma, not COPD
The LABA monotherapy boxed warning (increased asthma-related deaths) applies specifically to asthma. In COPD, LABA monotherapy is a standard and accepted maintenance therapy, as COPD bronchodilation does not carry this IgE/eosinophilic risk. Formoterol is indeed approved as a LABA for COPD (and asthma — always with ICS in asthma). LABA-LAMA combination is preferred in moderate-severe COPD but LABA monotherapy is appropriate in milder disease.
Anticholinergics: SAMA and LAMA
Anticholinergic (muscarinic antagonist) bronchodilators act by competitively blocking muscarinic M3 receptors on bronchial smooth muscle and submucosal glands, thereby preventing acetylcholine-mediated bronchoconstriction and mucus hypersecretion. Vagal tone is a significant contributor to resting airway resistance (particularly in COPD), making anticholinergics especially valuable in that condition. The two clinically important subcategories are short-acting muscarinic antagonists (SAMA) and long-acting muscarinic antagonists (LAMA).
Ipratropium (SAMA): Derived from atropine but designed as a quaternary ammonium compound, ipratropium has poor systemic absorption from inhaled or oral routes, dramatically limiting CNS and systemic anticholinergic effects. Onset: 15–30 minutes; duration: 4–6 hours. Uses: (a) acute severe asthma (combined with SABA via nebuliser in the emergency setting for additive bronchodilation — the two work on different receptors); (b) COPD — as rescue therapy and in mild stable COPD. ADRs: dry mouth (most common), throat irritation, urinary hesitancy (particularly in elderly males with BPH), acute angle-closure glaucoma if accidentally sprayed into the eyes (use mouthpiece, not face mask).
Tiotropium (LAMA): The prototype long-acting muscarinic antagonist. Mechanism: slow dissociation from M1/M3 receptors (rapid kinetics at M2 — preserves the M2-mediated presynaptic negative feedback that limits ACh release). Duration: 24 hours (once-daily). Clinical use: maintenance therapy in COPD — reduces exacerbation frequency, improves lung function and exercise tolerance; also approved as an add-on in severe asthma. Other LAMAs include glycopyrronium and umeclidinium (used in once-daily inhalers, often in LABA-LAMA fixed combinations such as indacaterol/glycopyrronium or vilanterol/umeclidinium). ADRs: dry mouth (most common and dose-limiting), constipation, urinary retention, blurred vision; less central effects than atropine due to poor CNS penetration.
| Agent | Class | Onset | Duration | Primary Use | Key ADR |
|---|---|---|---|---|---|
| Ipratropium | SAMA | 15–30 min | 4–6 h | Acute severe asthma + COPD rescue | Dry mouth, urinary hesitancy |
| Tiotropium | LAMA | 30 min | 24 h | COPD maintenance; severe asthma add-on | Dry mouth, constipation |
Inhaled Corticosteroids and Anti-inflammatory Agents
The anti-inflammatory agents for obstructive airway disease form a mechanistically diverse group. Their common thread is targeting the downstream inflammatory cascade rather than the bronchospasm itself — hence they require days to weeks for maximal effect and are maintenance (controller) rather than rescue agents. This group includes inhaled corticosteroids, leukotriene modifiers, methylxanthines, and the newer targeted biologics.
Inhaled corticosteroids (ICS): Agents include beclomethasone, budesonide, fluticasone, and mometasone. Mechanism: glucocorticoid receptor activation → reduced transcription of pro-inflammatory cytokines (IL-4, IL-5, TNF-α, GM-CSF), reduced eosinophil recruitment, reduced mucus secretion, reduced vascular permeability. In asthma, ICS is the cornerstone of maintenance therapy from Step 2 — no other controller reduces asthma-related mortality and morbidity as consistently. In COPD, ICS is added only selectively: for patients with ≥2 moderate exacerbations/year or ≥1 hospitalisation, or when blood eosinophils ≥300 cells/µL suggest eosinophilic overlap. ICS in COPD carries a clinically significant risk of pneumonia (meta-analysis data) — not a class effect in asthma at equivalent doses. Local ADRs: oral candidiasis (oropharyngeal deposition — prevented by rinsing mouth after use), dysphonia, reflex cough. Systemic ADRs at high doses: adrenal suppression, skin fragility, cataract.
Leukotriene modifiers:
- Montelukast and zafirlukast are selective CysLT1 receptor antagonists — they block the receptors for LTD4 and LTE4 on bronchial smooth muscle, preventing leukotriene-mediated bronchoconstriction and airway oedema. They do not inhibit leukotriene synthesis. Oral route; useful in aspirin-exacerbated asthma, exercise-induced asthma, and allergic rhinitis–asthma overlap. ADRs: generally well tolerated; montelukast carries an FDA black-box warning for neuropsychiatric events (depression, suicidal ideation, aggression) — counsel patients and reassess if psychiatric symptoms emerge.
- Zileuton inhibits 5-lipoxygenase (5-LOX), the enzyme that synthesises all leukotrienes, preventing their formation upstream. Hepatotoxicity risk; requires LFT monitoring. Less widely used than CysLT1 antagonists.
Theophylline (methylxanthine): Mechanism: inhibits phosphodiesterase (PDE) → ↑cAMP/cGMP → bronchodilation; also adenosine receptor antagonism (anti-inflammatory). Once the mainstay of asthma treatment; now a reserve agent due to its narrow therapeutic index (therapeutic range 5–15 µg/mL; toxicity begins ~20 µg/mL with seizures, arrhythmias). It is a CYP1A2 substrate: smoking induces CYP1A2, reducing theophylline levels in smokers (COPD patients who smoke need higher doses); erythromycin and fluoroquinolones inhibit CYP1A2, increasing levels to toxic range. Therapeutic drug monitoring (TDM) is mandatory.
Biologics for severe asthma:
| Agent | Target | Indication | Notes |
|---|---|---|---|
| Omalizumab | Anti-IgE | Moderate-severe allergic asthma, serum IgE 30–700 IU/mL | Anaphylaxis risk (observe 30 min post-injection) |
| Mepolizumab / Reslizumab | Anti-IL-5 | Severe eosinophilic asthma (blood eos ≥300/µL) | Reduces exacerbations; SC/IV |
| Benralizumab | Anti-IL-5Rα | Severe eosinophilic asthma | Depletes eosinophils via ADCC; every 8 weeks |
| Dupilumab | Anti-IL-4Rα | Moderate-severe type-2 asthma; also atopic dermatitis, rhinosinusitis | Blocks IL-4 and IL-13 signalling; SC |
All biologics: reserve for Step 4–5 severe asthma uncontrolled on high-dose ICS-LABA. Patient selection based on biomarkers (eosinophil count, IgE level, fraction of exhaled NO).
SELF-CHECK
A patient with aspirin-exacerbated asthma and co-existing allergic rhinitis would benefit most from which leukotriene modifier, and through which mechanism?
A. Zileuton — inhibits 5-LOX, preventing all leukotriene synthesis including the excess LTE4 driving aspirin-exacerbated bronchoconstriction
B. Montelukast — blocks CysLT1 receptors, preventing LTD4/LTE4-mediated bronchoconstriction; also approved for allergic rhinitis
C. Both agents are equally effective because both block the final common pathway of leukotriene-mediated bronchoconstriction
D. Neither — leukotriene modifiers are ineffective in aspirin-exacerbated asthma because the mechanism is COX-2 inhibition
Reveal Answer
Answer: B. Montelukast — blocks CysLT1 receptors, preventing LTD4/LTE4-mediated bronchoconstriction; also approved for allergic rhinitis
Montelukast is the preferred leukotriene modifier for aspirin-exacerbated asthma (AEA) in clinical guidelines. In AEA, COX inhibition by aspirin/NSAIDs shunts arachidonic acid toward the 5-LOX pathway, causing excess cysteinyl leukotriene production. Montelukast (CysLT1 receptor antagonist) blocks the downstream bronchospastic and inflammatory effects of these leukotrienes. Crucially, montelukast is also approved for allergic rhinitis — making it the single best agent for this patient's combined AEA and rhinitis. Zileuton (5-LOX inhibitor) targets synthesis upstream but carries hepatotoxicity risk and requires LFT monitoring; it is less commonly used in practice. The key distinction: montelukast/zafirlukast = receptor blockade; zileuton = synthesis inhibition — a frequent exam topic.