Page 3 of 13
PH5.1 | PH5.1 | Obstructive Airway Disease Pharmacotherapy — SDL Guide (Part 3)
Rhinitis Pharmacotherapy
Allergic rhinitis pharmacotherapy deserves dedicated attention not only because it is a common standalone condition but because under-treated rhinitis is a major trigger for exacerbations of co-existing asthma. The 'united airway' model holds that the upper and lower airways share a continuous epithelium and inflammatory milieu — nasal inflammation from untreated rhinitis causes post-nasal drip, triggers bronchial hyper-reactivity, and perpetuates IgE sensitisation. Therefore, optimising rhinitis management often reduces the burden on lower-airway controllers.
The most effective single drug class for allergic rhinitis is intranasal corticosteroids (INCS) — including fluticasone furoate, mometasone furoate, budesonide, and beclomethasone nasal sprays. They reduce all four symptom domains: nasal congestion, rhinorrhoea, sneezing, and pruritus. This is the class that antihistamines cannot match for congestion (the most burdensome symptom for many patients). Onset is gradual — full effect in 1–2 weeks; maximal effect with regular use. ADRs: local — nasal dryness, epistaxis (especially if pointed toward the septum; correct technique directs spray laterally); systemic effects minimal with modern agents at recommended doses.
Second-generation H1 antihistamines: Cetirizine (mildly sedating, active metabolite levocetirizine), loratadine (non-sedating, active metabolite desloratadine), and fexofenadine (non-sedating, P-gp substrate, not metabolised to active form). Mechanism: inverse agonism at H1 receptors on nasal mucosal vasculature and mucus glands. Effective for sneezing, pruritus, rhinorrhoea but not for nasal congestion (histamine plays a minor role in nasal vascular tone; alpha-adrenergic and H3-receptor mechanisms dominate congestion). First-generation antihistamines (diphenhydramine, promethazine) cause significant sedation, impair psychomotor function, and are anticholinergic — avoid for rhinitis in functioning adults.
Decongestants: Topical agents (oxymetazoline, xylometazoline) are alpha-1/alpha-2 agonists that cause nasal mucosal vasoconstriction. Highly effective for acute congestion within minutes; but use must be strictly limited to ≤5 days — prolonged use causes rebound congestion (rhinitis medicamentosa) from receptor downregulation and mucosal reactive hyperaemia. Oral pseudoephedrine is longer-acting but causes systemic vasoconstriction (contraindicated in hypertension, cardiovascular disease) and is regulated as a precursor for methamphetamine synthesis.
Cromolyn sodium (sodium cromoglycate): Mast cell stabiliser; prevents degranulation and mediator release. Requires 4× daily use; less effective than INCS; but has an excellent safety profile and is preferred in pregnancy (category B) and young children. Also available as eye drops for allergic conjunctivitis.
CLINICAL PEARL
The asthma–LABA safety rule is probably the highest-stakes drug safety fact in this module. Internalize it as a conditional: in asthma, LABA + ICS = standard care; LABA alone = contraindicated (boxed warning: increased asthma-related deaths, demonstrated in the SMART trial). In COPD, there is no such restriction — LABA monotherapy is a core maintenance strategy. The mechanism behind this difference is that LABA without ICS in asthma fails to attenuate the eosinophilic inflammation and remodelling that drives progressive disease; the patient 'feels fine' while the underlying disease worsens. Contrast this with COPD, where the dominant pathology (neutrophilic/macrophage inflammation) is not substantially attenuated by ICS anyway, and bronchodilation directly addresses the primary functional impairment.
A second high-yield safety fact: rhinitis medicamentosa from topical decongestants. Never prescribe or recommend topical decongestants for more than 5 days. When patients present with worsening nasal congestion despite using a decongestant spray, ask how long they have been using it — the 'treatment' may be the cause of their rebound symptoms.
For theophylline: always check the patient's smoking status and current medications before prescribing. Smokers have dramatically lower theophylline levels (CYP1A2 induction). Starting antibiotics (erythromycin, fluoroquinolones) in a patient on theophylline can cause toxicity within days — check for this interaction every time.
Clinical Decision-Making in Obstructive Airway Disease
Clinical pharmacology is only complete when the drug knowledge translates into a structured management algorithm that a clinician can apply at the bedside. The evidence-based frameworks for asthma and COPD are internationally agreed upon and updated regularly — they represent the highest-quality synthesis of randomised controlled trial evidence and real-world effectiveness data. Learning these frameworks is not about memorising a list of steps; it is about understanding the underlying logic: why bronchodilators precede ICS in COPD, why biologics appear only at Step 5 in asthma, and why acute exacerbations require a fundamentally different approach from maintenance therapy. These frameworks also provide the benchmark against which any deviation (due to patient preference, comorbidity, or resource constraints) must be explicitly justified. Mastery here means being able to explain the rationale for each step, not merely recall the drugs.
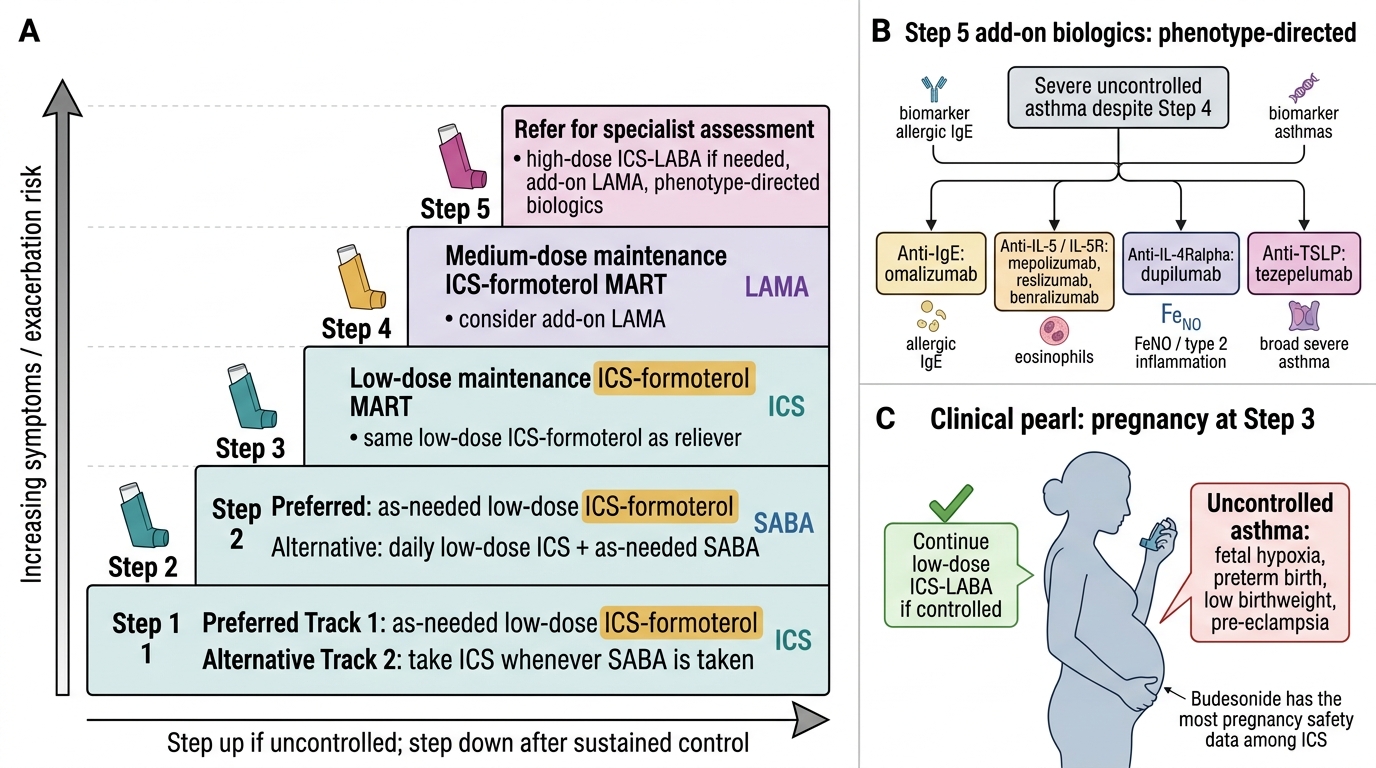
Stepwise management of asthma (GINA): Asthma therapy is titrated up (step-up) when control is inadequate and stepped down when control is maintained for ≥3 months. The five GINA steps are:
- Step 1 (mild intermittent): as-needed low-dose ICS-formoterol (preferred MART strategy) or SABA reliever alone.
- Step 2 (mild persistent): daily low-dose ICS + as-needed SABA reliever. Alternative: LTRA (less effective than ICS).
- Step 3 (moderate persistent): low-dose ICS-LABA combination (fixed or MART). Note: LABA must always accompany ICS — this step is NOT LABA monotherapy.
- Step 4 (severe persistent): medium/high-dose ICS-LABA. Add-on tiotropium (LAMA), LTRA, or theophylline. Consider referral to specialist.
- Step 5 (very severe / refractory): specialist-guided. Add-on biologics (omalizumab for allergic, mepolizumab/benralizumab/reslizumab for eosinophilic, dupilumab for type-2 inflammation). Oral corticosteroids only as last resort (significant systemic toxicity).
Acute severe asthma protocol: First-line: high-dose SABA via nebuliser (salbutamol 2.5–5 mg every 20 min) + ipratropium nebuliser (additive bronchodilation via different receptor) + systemic corticosteroids (prednisolone oral or IV hydrocortisone). Oxygen for SpO2 ≥94%. Reassess peak flow every 15–30 min. ICU criteria: SpO2 <92%, silent chest, exhaustion, rising PaCO2.
COPD management (GOLD ABCD): The GOLD 2023 framework classifies patients by symptom burden (mMRC dyspnoea scale/CAT score) and exacerbation risk into Groups A, B, E:
- Group A (few symptoms, low risk): SABA or SAMA on demand; consider single long-acting bronchodilator.
- Group B (more symptoms, low risk): LABA or LAMA (LABA-LAMA preferred if mMRC ≥2).
- Group E (high exacerbation risk): LABA-LAMA first; add ICS if eosinophils ≥300/µL; consider roflumilast if FEV1 <50%, chronic bronchitis phenotype.
Special populations:
- Pregnancy: SABA and ICS (budesonide has best safety data) are safe and essential — uncontrolled asthma is more dangerous to the fetus than inhaled drugs. Theophylline may be used but levels must be monitored closely. Biologics: insufficient data; use only if no alternative.
- Paediatrics: SABA safe at all ages. ICS from age 5 (growth concerns at high doses — use lowest effective dose). Montelukast (oral) is useful from age 6 months for allergic rhinitis and mild asthma. LABAs approved from age 5 (with ICS). Biologics: mepolizumab from age 6.
Monitoring points:
- ICS: check inhaler technique, mouth rinse compliance; ask about hoarseness/dysphonia.
- Theophylline: TDM (target 5–15 µg/mL), ask about new medications (CYP1A2 interactions) and smoking status changes.
- Biologics: pre-injection eosinophil count and IgE level; for omalizumab, observe 30 min post-injection for anaphylaxis.
GINA Stepwise Asthma Management Ladder
SELF-CHECK
A 30-year-old woman with moderate persistent asthma (GINA Step 3) is well-controlled on low-dose ICS-LABA for 4 months. She is now 8 weeks pregnant. What is the most appropriate management?
A. Discontinue the LABA immediately — all LABA are contraindicated in pregnancy
B. Switch to theophylline — it is safer than inhaled agents in pregnancy
C. Continue low-dose ICS-LABA; uncontrolled asthma carries more risk to the fetus than inhaled therapy
D. Stop all controller therapy and use SABA only — the safest approach in pregnancy
Reveal Answer
Answer: C. Continue low-dose ICS-LABA; uncontrolled asthma carries more risk to the fetus than inhaled therapy
Uncontrolled asthma in pregnancy is associated with preterm birth, low birthweight, pre-eclampsia, and fetal hypoxia — all of which are more dangerous to the fetus than inhaled corticosteroids and LABAs at standard doses. Budesonide has the best pregnancy safety data among ICS. ICS-LABA is the recommended maintenance therapy for GINA Step 3 in pregnancy. Stopping controllers risks exacerbations. Theophylline requires close TDM in pregnancy due to changed kinetics and has a narrow therapeutic index — it is not preferred over ICS-LABA.
Self-Assessment: Obstructive Airway Disease Pharmacotherapy
Consolidate your learning by working through these clinical scenarios. For each question, formulate your answer before reading the key points. These scenarios are designed to test application (Bloom's level 3) and analysis (Bloom's level 4) — the competency level required for PH5.1.
Scenario 1: A 55-year-old COPD patient (GOLD Group B, FEV1 60% predicted) is already on tiotropium (LAMA) once daily. His dyspnoea remains significant on exertion. What is the rational next step in pharmacotherapy and why?
Key reasoning: LABA-LAMA combination provides superior bronchodilation to either agent alone in GOLD Group B with inadequate symptom control. Adding a LABA (e.g., indacaterol or formoterol) creates dual bronchodilation via different receptor mechanisms. ICS is not the next step here — blood eosinophil count would need to be ≥300/µL or exacerbation frequency high (GOLD Group E criteria). This is a common prescribing error to avoid.
Scenario 2: A student nurse asks you: 'Why do patients with rhinitis often have worse asthma control in spring?' How do you explain the united airway concept and what pharmacological intervention addresses both conditions?
Key reasoning: Allergic rhinitis and asthma share IgE-mediated pathophysiology and the same allergen exposure. Nasal inflammation produces post-nasal drip, direct aspiration of inflammatory mediators, and neurogenic reflexes that increase bronchial hyperreactivity. Untreated rhinitis impairs nasal filtration and humidification, allowing more allergens and cold air to reach the lower airway. Pharmacological intervention: treating rhinitis with INCS plus a 2nd-gen antihistamine (to address all symptom domains including congestion) can measurably reduce asthma exacerbation frequency.
Scenario 3: Explain why two patients on theophylline maintenance therapy — a 60-year-old COPD patient who smokes 20 cigarettes/day versus a 60-year-old who does not smoke — may require very different theophylline doses.
Key reasoning: Smoking induces CYP1A2, the primary hepatic enzyme responsible for theophylline metabolism. In the smoker, increased CYP1A2 activity accelerates theophylline clearance, lowering plasma levels — requiring higher doses to achieve the therapeutic window (5–15 µg/mL). The non-smoker metabolises theophylline more slowly; the same dose would produce higher plasma levels and potential toxicity. If the smoking patient stops smoking (e.g., hospitalisation), CYP1A2 induction reverses within days to weeks, and the previously-adequate theophylline dose can become toxic. This must trigger TDM and dose reduction.